TLDR:
Spinal cord stimulation is not a last resort, it does not mean permanent commitment, and most patients go home the same day as their trial. The device does not replace your spinal cord and is fully reversible. Insurance often covers it, and most people with prior back surgery are still candidates. If you have been told SCS is “too extreme” or “not for people like you,” read on.
A lot of patients come to us having already dismissed spinal cord stimulation as an option, and when we ask why, the reasons are almost always based on things they heard, not things they were told by a doctor who actually evaluated them.
That matters, because SCS has one of the stronger evidence bases in interventional pain medicine. For conditions like CRPS, sciatica, and failed back surgery syndrome, it can produce meaningful relief when other treatments have stopped working.
So here are seven things patients get wrong, and what the evidence actually says.
1. “It sounds too extreme. I am not ready for something that invasive.”
This is the most common hesitation we hear, and it is worth unpacking.
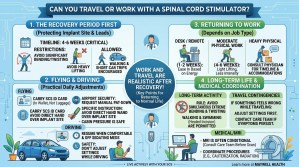
The trial phase of spinal cord stimulation is minimally invasive. Thin leads are placed near the spinal cord using a needle, similar to how an epidural steroid injection is performed. No incision, no stitches, no general anesthesia in most cases. You go home the same day.
The trial lasts about a week. You try it. If it works, you move forward with a permanent implant. If it does not, the leads are simply removed. There is nothing permanent about the first step.
The permanent implant is a real procedure, but it is outpatient for most patients. The device sits under the skin, not inside your spinal canal. “Invasive” is a relative term, and compared to major spinal surgery, this does not belong in the same category.
2. “I already had back surgery. That probably rules me out.”
Actually, the opposite is often true.
Failed back surgery syndrome, meaning ongoing pain after one or more spinal procedures, is one of the most well-studied indications for SCS. Patients who had microdiscectomy, lumbar fusion, or decompression for spinal stenosis and are still in pain are frequently good candidates.
Prior surgery does not automatically disqualify you. Your anatomy matters, your pain pattern matters, and your overall health matters. But the history of a prior procedure is not a dealbreaker. We evaluate each patient individually.
If you have had surgery and are still struggling, contact us to find out whether SCS is worth discussing.
3. “If it does not work, I am stuck with it.”
This one needs to be said plainly: spinal cord stimulators are removable.
The device can be turned off, adjusted, and explanted. This is not an irreversible commitment. The trial period exists specifically so you can evaluate the therapy before any permanent hardware is placed. Patients who do not get adequate relief during the trial do not proceed to implantation.
Even after permanent implantation, if your situation changes, the device can be removed. It is designed to be a long-term option, not a one-way door.
4. “I heard it completely blocks the pain signal. What does that do to my body?”
Spinal cord stimulation does not block pain signals in the way people sometimes imagine.
It does not cut off sensation, it does not numb your limbs, and it does not interfere with normal body function. What it does is modulate how the spinal cord processes pain signals before they reach the brain. Depending on the stimulation type, patients may feel a mild tingling (paresthesia-based stimulation) or nothing at all (sub-perception stimulation, which is common with newer devices).
You can still feel temperature, touch, and pressure normally. The device targets the pain pathways, not your sensory system as a whole. This is very different from what patients sometimes imagine when they picture something “going into the spine.”
5. “My pain is in my SI joint and lower back, not really my legs. Is this even relevant for me?”
SCS is sometimes associated primarily with leg pain, but it covers more ground than that.
For patients with sacroiliac joint pain, peripheral nerve stimulation may actually be a more targeted option. But SCS itself has been used effectively for axial low back pain as well, particularly with newer waveform technologies like high-frequency and burst stimulation.
If you are dealing with SI joint pain and wondering whether interventional options are worth exploring, we also offer sacroiliac joint steroid injections and SI joint fusion for appropriate candidates. The right path depends on your specific diagnosis, which is why a proper evaluation matters.
6. “Insurance will never cover something like this.”
Many patients assume SCS is experimental or elective and therefore out of pocket. That is not accurate.
Spinal cord stimulation has FDA approval and is covered by Medicare and most major commercial insurers for approved indications. Coverage typically requires documentation of failed conservative treatment, including medications and other interventional procedures, along with a psychiatric or psychological evaluation and successful trial.
The process takes time and requires paperwork, yes. But for patients who meet criteria, this is not an out-of-pocket expense. Our team can walk you through what your specific coverage looks like.
7. “I do not want to become dependent on another medical device.”
This concern makes sense, but it is worth examining what dependence actually means here.
Many patients asking this question are already taking daily medications, some of which carry real risks of physical dependence. SCS, by contrast, does not involve anything pharmacological. It does not affect your liver, kidneys, or brain chemistry. You can turn it off. You can reduce settings. You can stop using it entirely if you choose.
For some patients, SCS significantly reduces or eliminates the need for opioid medications. That is one of the reasons it is increasingly considered earlier in treatment rather than only as a last resort. Some patients also benefit from combining SCS with other approaches like ketamine therapy, particularly for complex pain conditions like CRPS or when sensitization is part of the picture.
If medication dependence is something you are trying to move away from, SCS may actually be worth a conversation sooner rather than later.
The Bottom Line
Spinal cord stimulation is not right for everyone. No treatment is. But many of the reasons patients rule it out before they are even evaluated are based on misunderstandings, not medical facts.
If you have been living with chronic pain that is not responding to other treatments, and you have questions about whether SCS is appropriate for your situation, we are here to talk through it.
You can also learn more about what we treat at MayWell Health, including conditions like arthritis and spinal stenosis that often lead patients toward considering advanced interventional options.