TLDR CRPS produces pain that is wildly disproportionate to the original injury, often described as burning, stabbing, or electric. The affected limb can change color, temperature, and appearance. Clothing touching your skin can feel unbearable. Most patients with CRPS have been dismissed, misdiagnosed, or told the pain is psychological before they get an accurate diagnosis. It is not. It is a real, documented condition with real treatment options.
There is a particular kind of exhaustion that comes with having a condition most people have never heard of.
You hurt constantly. The pain is unlike anything you experienced before the injury that started it, which might have been something minor, a sprained ankle, a broken wrist, a routine surgery. The injury healed, or should have healed, but the pain did not go away. It got worse. And when you try to explain it to people, including some doctors, you watch their faces and know they are not quite believing you.
That is complex regional pain syndrome. And if that paragraph described your last two years, you are not imagining it.
The Pain Itself
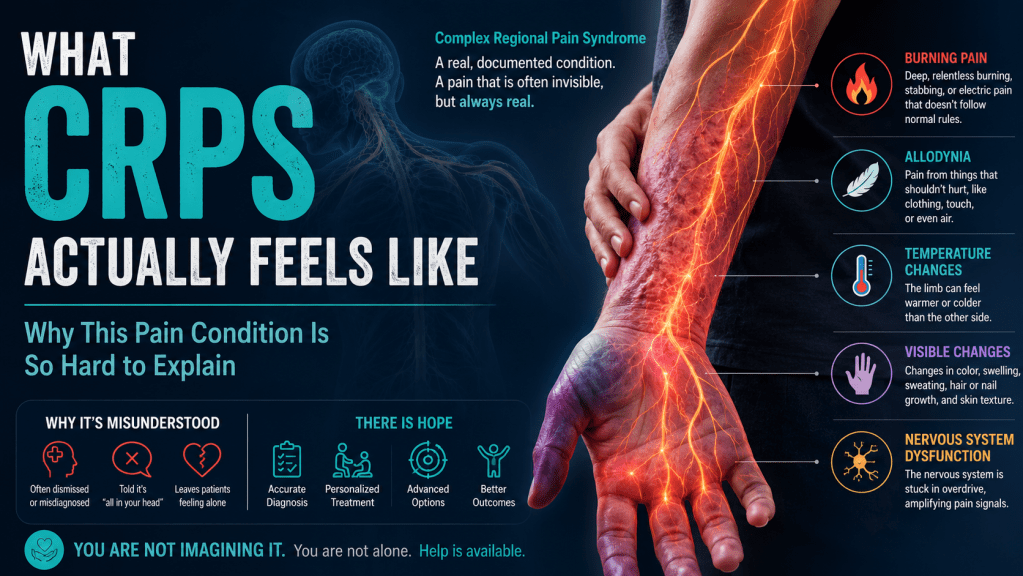
The most common description patients use is burning. A deep, relentless burning in the affected limb that does not behave the way normal pain does.
Normal pain has a logic to it. You move wrong and it spikes. You rest and it eases. CRPS does not follow that logic. The pain can be severe when you are completely still. It can be triggered by things that should not hurt at all. The weight of a bedsheet. Air moving across your skin. Someone brushing your arm in passing.
That last phenomenon has a name: allodynia. It means pain from stimuli that are not normally painful. Patients with CRPS describe pulling their sleeves down carefully so fabric does not touch the affected area, sleeping with the limb uncovered because contact is unbearable, avoiding crowded spaces because accidental contact is too risky. This is not sensitivity or low pain tolerance. It is a nervous system that has fundamentally changed how it processes signals.
There is also hyperalgesia, which means that things that are slightly painful become dramatically more painful. A minor bump that would register as a two becomes an eight. The volume is turned up and it does not turn back down.
What It Looks Like From the Outside
CRPS is unusual among pain conditions because it often produces visible changes in the affected limb.
The skin can change color, cycling through red, purple, pale, or blotchy depending on the stage and the individual. Temperature changes are common, the limb feels noticeably warmer or colder than the other side. Swelling is common early in the condition. Some patients notice changes in hair and nail growth on the affected side. In longer-standing cases, the skin can take on a shiny or thinned appearance.
These changes are why CRPS was historically called reflex sympathetic dystrophy. The sympathetic nervous system, which controls things like blood vessel tone and skin temperature, is involved in producing many of these visible signs.
The visible component matters for patients because it is one of the few things that can make invisible pain visible to the people around them. But not everyone with CRPS has dramatic visible changes, and the absence of them does not mean the pain is any less real.
The Emotional Weight of It
This part gets left out of clinical descriptions, so it is worth saying plainly.
CRPS is demoralizing in a specific way. It often starts from something that should have been minor. Patients cycle through anger at the original injury, confusion about why they are not getting better, and eventually a grinding grief for the life they had before. Sleep is disrupted because pain does not stop at night. Work becomes difficult or impossible depending on the job. Relationships strain under the weight of a condition that is hard to explain and harder to watch.
Many patients arrive at a CRPS diagnosis after months or years of being told their pain was exaggerated, psychosomatic, or drug-seeking. That history leaves a mark. It makes patients cautious about seeking care, skeptical of new physicians, and sometimes reluctant to describe the full extent of what they are experiencing for fear of not being believed again.
If that is where you are, it is worth saying directly: CRPS is a recognized medical diagnosis with a published diagnostic criteria set. The pain is real. The nervous system changes are measurable. The condition is taken seriously by pain specialists.
Why It Develops
The honest answer is that medicine does not fully understand why some people develop CRPS after an injury and others do not.
What is understood is that in CRPS, the nervous system’s response to an injury does not resolve the way it should. The inflammatory response, the sympathetic nervous system activity, and the central sensitization that normally quiet down after an injury instead persist and amplify. The result is a pain state that has become self-sustaining, no longer tied to ongoing tissue damage but driven by a nervous system that is stuck in alarm mode.
The triggering injury is often minor. Fractures, sprains, surgeries, and even needle sticks have been documented as CRPS triggers. In rare cases there is no identifiable injury at all. The severity of the original injury does not predict whether CRPS develops or how severe it becomes.
What Happens Without Treatment
CRPS does not reliably resolve on its own, particularly when it has been present for more than a few months.
In the early stages, some patients do recover with aggressive physical therapy and pain management. The longer the condition persists without adequate treatment, the more entrenched the central sensitization becomes and the harder it is to reverse.
Some patients develop spread, meaning the condition extends beyond the original limb to other areas of the body. Some develop significant mobility loss in the affected limb as a result of guarding and disuse over time. The condition can be destabilizing in ways that go well beyond the physical, affecting mental health, employment, and independence.
This is why early diagnosis and treatment matter more for CRPS than for many other pain conditions.
What Treatment Actually Looks Like
There is no single treatment that works for everyone with CRPS, and anyone who tells you otherwise is not being honest with you.
What has the strongest evidence is a combination approach. Physical and occupational therapy to maintain function in the affected limb, even when movement is painful, because disuse worsens the condition over time. Pain medication to make therapy tolerable. And interventional treatments to address the underlying nervous system dysfunction.
Spinal cord stimulation has one of the strongest evidence bases for CRPS of any interventional treatment. Multiple controlled trials have shown meaningful, durable pain reduction in CRPS patients who did not respond to conservative treatment. It is not a cure, but for many patients it is the difference between a life that functions and one that does not.
Peripheral nerve stimulation is another option for patients with CRPS affecting a specific limb or nerve territory. Depending on where the condition is located, targeted peripheral stimulation may be more precise and equally effective.
Ketamine therapy is used for CRPS patients where central sensitization is a major driver of the pain. Ketamine works through a different mechanism than stimulation therapies, blocking NMDA receptors involved in the sensitization process. For patients who have not responded adequately to other approaches, it is a legitimate option with a growing evidence base in refractory CRPS.
Epidural steroid injections and sympathetic nerve blocks are sometimes used earlier in the treatment course, particularly in the acute phase when inflammatory activity is high.
What We See in Our Practice
Patients with CRPS who come to us have almost always had a long road before they arrive. Multiple providers, multiple failed treatments, and a diagnosis that came later than it should have.
The patients who do best are generally those who engage with physical therapy alongside their interventional treatment, who have realistic expectations about what any single treatment can accomplish, and who have a care team that understands CRPS specifically rather than treating it like generic back pain.
CRPS is not generic back pain. It is a distinct neurological condition that requires a physician who understands the difference.
If You Are Trying to Figure Out Whether This Is What You Have
The diagnostic criteria for CRPS, the Budapest Criteria, require ongoing pain disproportionate to the original injury plus a combination of sensory, vasomotor, sudomotor, and motor or trophic signs and symptoms in at least two categories.
In plain terms: severe burning pain, plus some combination of skin color or temperature changes, swelling, sweating abnormalities, or movement difficulties, in the area that was injured.
If that sounds like your situation and you have not had a formal evaluation, contact us. The sooner CRPS is accurately diagnosed and treated, the better the outcomes tend to be.
You can learn more about the condition and how we approach it at MayWell Health, and about the full range of treatments we offer at MayWell Health.