TLDR:
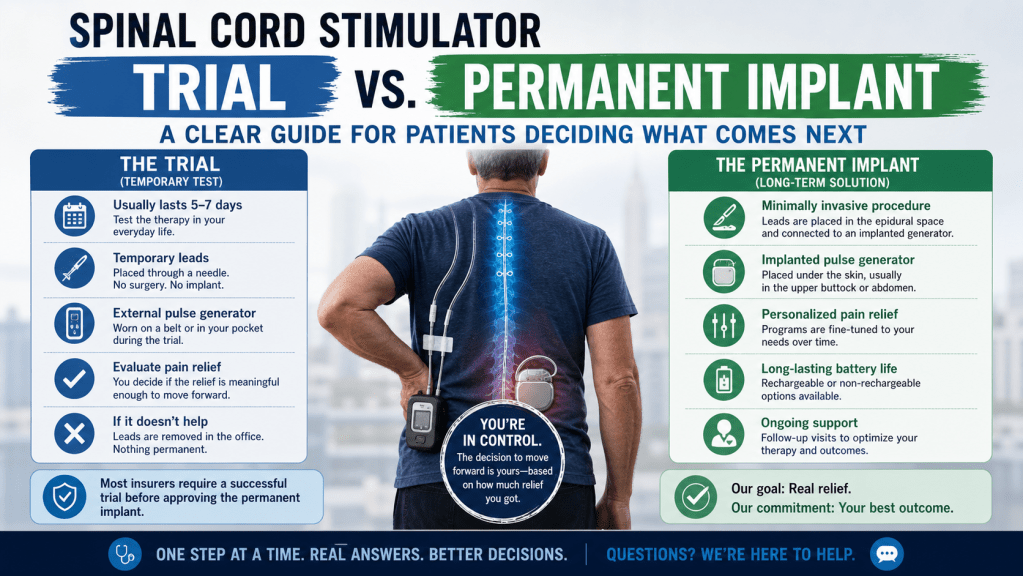
The trial is a temporary test run, usually 5 to 7 days, where leads are placed without a full implant to see if the therapy actually helps your pain. If it does, you move to the permanent implant. If it does not, the leads are removed and nothing permanent has been done to your body. Most insurers require a successful trial before approving the permanent device. The decision to move forward is yours, based on how much relief you got.
One of the things that makes spinal cord stimulation different from most pain treatments is the built-in test period. You do not have to commit to anything permanent upfront. You try it first.
That is genuinely unusual in medicine, and it is worth understanding properly before you go into any appointments. A lot of patients arrive confused about what the trial actually involves, whether it hurts, what counts as success, and what happens next. This piece answers those questions directly.
What the Trial Actually Is
The trial is a short-term test of spinal cord stimulation, typically lasting 5 to 7 days, designed to tell you and your physician whether this therapy meaningfully reduces your pain.
During the trial, thin electrode leads are placed near your spinal cord using a needle-based approach, similar in technique to how an epidural steroid injection is performed. There is no surgical incision. No pulse generator is implanted. The leads exit through the skin and connect to an external device you wear or carry during the trial period.
You go home. You live your normal life as much as your recovery allows. You track your pain levels. After the trial period, you come back, the leads are removed, and you have a real data point: did this help or not?
That is it. No permanent hardware, no general anesthesia, no stitches.
What the Trial Feels Like
Most patients describe the placement procedure as uncomfortable but tolerable. Local anesthesia is used at the insertion site. Some patients receive mild sedation as well, though the procedure is typically done with you awake enough to provide feedback on lead placement, since your input helps guide positioning.
During the trial week itself, you will feel stimulation effects depending on the device type. Older stimulation patterns produce a mild tingling sensation in the area where you feel pain. Newer high-frequency and burst stimulation modes often produce no sensation at all, which surprises patients who expect to feel something obvious.
You will be asked to limit certain movements during the trial, particularly bending and twisting, to keep the leads stable. This is temporary. The goal is to get a clean read on whether the stimulation helps, not to restrict your life permanently.
What Counts as a Successful Trial
Most physicians and insurers use 50% or greater pain reduction as the threshold for a successful trial. That is the clinical benchmark, but it is not the only thing that matters.
Your physician will also want to know whether your function improved. Could you sleep better? Walk further? Reduce your pain medication? These things matter alongside the raw pain score.
Be honest during your trial evaluation. Patients sometimes feel pressure to report success when they are uncertain, either because they want to move forward or because they do not want to disappoint anyone. That pressure works against you. If the relief was partial, say so. If it was in a different area than expected, say so. That information helps your physician adjust lead placement or stimulation settings before you commit to anything permanent.
A trial that shows partial benefit is still useful information. It is not automatically a failure. Your physician may suggest adjustments and a repeat trial, or may recommend a different approach entirely based on what you reported.
What Happens If the Trial Does Not Work
The leads are removed. That is the whole point of the trial design.
Nothing permanent has been placed in your body. You are back to where you started medically, with more information than you had before. If SCS is not the right fit, your physician can discuss other options. For patients with sacroiliac joint pain, that might mean evaluating SI joint fusion or a sacroiliac joint steroid injection. For patients with significant back pain who have had prior surgery, lumbar fusion may be worth reconsidering. For conditions involving nerve sensitization like CRPS, ketamine therapy is another avenue.
A failed trial does not close doors. It narrows the list, which is useful.
Moving to the Permanent Implant – What Changes
If your trial is successful, the next step is the permanent implant. Here is what is different.
The leads are placed more definitively, often through a small incision rather than purely via needle, to ensure long-term stability. A pulse generator, roughly the size of a large matchbox, is implanted under the skin, typically in the upper buttock or lower abdomen area. This is where the permanent procedure is meaningfully more involved than the trial.
The permanent implant is an outpatient surgical procedure for most patients. General anesthesia or deep sedation is more common at this stage than during the trial. You will have a small incision, a recovery period of a few weeks, and activity restrictions during healing.
The permanent device is rechargeable in most modern systems. Charging sessions are brief and happen every few days to a few weeks depending on your usage settings. The battery lasts years before the generator itself needs replacement, which is a separate minor procedure when the time comes.
The Decision Conversation – What to Actually Think About
Patients sometimes treat the decision to proceed to permanent implant as something the physician decides. It is not. You are the one who lived through the trial week. Your physician can tell you whether the data supports moving forward, but the decision is yours.
A few things worth thinking through honestly before that conversation:
Was the relief meaningful to you, not just measurable? A 50% reduction on a pain scale sounds significant. Whether it translated to real changes in how you lived that week is a separate question. Both matter.
Were there things you could do during the trial that you could not do before? Function is often a better measure than pain scores. If you slept through the night for the first time in months, that means something.
Did the stimulation cover the right areas? Sometimes the lead placement during a trial does not perfectly match your pain distribution. This can often be improved in the permanent procedure with more precise positioning.
Are you comfortable with the permanent procedure? The implant involves a real surgical step. If you have concerns about anesthesia, scarring, or recovery, raise them before you agree to a date. These are answerable questions.
What is your alternative? This is worth thinking about plainly. If the trial gave you meaningful relief and you decline the permanent implant, what is the plan? Continuing with medications that are not working well, or revisiting options that have already been tried, is a real cost. Weigh it honestly.
Who Is a Candidate for Each Step
Not everyone who comes to us asking about SCS will move directly to a trial. The evaluation process matters.
Patients with sciatica that has not responded to conservative treatment, persistent pain following spinal procedures, spinal stenosis without good surgical options, and conditions like CRPS and arthritis-related chronic pain are among those for whom SCS is worth evaluating.
The evaluation typically involves a review of your imaging and prior treatments, a discussion of what has and has not helped, and often a psychological evaluation, which is a standard requirement for insurers and a genuinely useful step for patients, not a hoop to jump through.
If you are earlier in your pain journey and wondering whether SCS is even on the table for you, reach out to us. The answer depends on your specific history and diagnosis, not on a general checklist.
The Short Version
The trial exists so you do not have to guess. It gives you real information about whether this therapy works for your pain, in your body, before anything permanent is placed.
If it works, you have a clear path forward. If it does not, you have ruled something out without lasting consequences.
The permanent implant is a meaningful step up in terms of procedure complexity, but it is also the step that delivers long-term relief for patients who responded well during the trial.
If you have questions about where you are in this process, or whether a trial makes sense for your situation, we are here to talk through it. You can learn more about what we do at MayWell Health.